Psychiatry was a roller coaster ride to me. I was somehow lacking of passion, reluctant to go to ward, clinic etc. And my EOP long case was a total nightmare for me, when I couldn't answer what's the dsm 5 criteria of OCD. (my patient had a triple diagnosis of MDD, GAD & OCD!!) Towards the last few weeks, I sorta developed some emotional attachment to some of the patients there, and I felt very bad for them. Anyway, psychiatry is indeed a 'major' posting(in fact no posting should be treated as minor!), you can totally be given a psychiatry long case in your mbbs finals, and mental health is a rising problem, whereby it's gonna be one of the top 3 disabilities in terms of global health issues.
First of all, history taking and physical examination.
Learning to take a history from a psychiatry patient can be very daunting at first. Imagine trying to ask about past medical history from a patient who will talk to you about how he is the son of god or he can fly instead. or how a disinhibited patient can possibly masturbate in front of you. But all these should not be the reasons for you to back off, instead, these are exactly the features that you want to pick up!
For example, a patient who tells you that he is a god who is omnipotent, you needa pick up that he has grandiosity. If a patient tells you that there are unknown forces hitting on him, think of somatic passivity.
One unique aspect of of psychiatry is that you have to perform mental status examination(MSE) on every patients. It is an assessment to find out if the patient is currently suffering from any active psychosis, assess suicide risk etc. All the components can be found in a psychiatry clerking sheet.
Patient's insight on his condition is particularly important in a psychiatry history as well.
Another thing that is important in psychiatry is the assessment of patient's 'affect'.
'Mood' is something that the patient tells you. For example: I am having a bad mood today.
Affect on the other hand, is something objective, it is what you think the patient's mood is based on observation.
Understand the meaning of psychopathology. They are terms that describe what is the patient's problems or rather, experience. For example: somatic passivity, derogatory delusion, tangentiality, delusional perception, etc.
Definitions are very important. For example: Illusion vs Hallucination. Delusion, psychosis, etc. Some definitions are based on the DSM 5 criterias. For example, mania vs hypomania.
Here comes the Important Topics in psychiatry:
1) Psychotic Conditions:
Schizophrenia, Schizoaffective, Schizophreniform, Brief Psychotic disorder,
Drug-induced psychosis
Mx: basically antipsychotics. Study about typical(first gen) vs atypical(sec gen) antipsychotics.
Read about the Schneider's First Rank Symptoms of Schizophrenia(important!)
Read about extrapyramidal side effects of first gen antipsycotics.
Read about Clozapine and its side effects.
Read about indications for ECT(electroconvulsive therapy).
2) Mood Disorders:
Bipolar 1, Bipolar 2, Major Depressive Disorder(MDD),
Mx: basically mood stabilisers for bipolar and antidepressants for MDD
Read about mood stabilisers and their side effects(lithium, sodium valproate, etc)
Lithium is interesting because although being the gold standard but
its toxicity is harzadous and narrow therapeutic index.
Read about all the classes of antidepressants(SSRI, SNRI, NaSSa, etc)
Please memorise how to assess suicide risk, using the sad person scale.
It is particularly important, as you can fail for not assessing it.
3) Anxiety, Phobia, Stress related disorders:
Generalised Anxiety Disorder(GAD),
Acute Stress Disorder, Adjustment Disorder, Post Traumatic Stress Disorder(PTSD)
Panic Disorders(Agoraphobia, specific phobias)
Obsessive Compulsive Disorder(OCD)
Aiyo so many, please hafal DSM 5 la haha.
4) Substance
Alcohol, Opioid, Stimulants(coccaine, amphetamine, cannabis), Nicotine, Caffeine
read about acetaldehyde dehydrogenase. Don't forget about CAGE questionnaire
Opioid is very important. Read about what are the drugs to treat.
Read about methadone replacement therapy.
Basically there are only three diagnoses that you can make;
a) Bla Use Disorder b) Bla Intoxication c) Bla withdrawal
whereby all are based on DSM 5.
Different substances give you different intoxication features.
For example, stimulants cause pupillary dilatation(mydriasis)
whereas opioids causes pupillary constriction(miosis) but overdose cause dilation due to anoxia instead.
So, have to really remember.
5) Eating Disorders
Anorexia Nervosa, Bulimia Nervosa
They have their respective DSM 5 criterias.
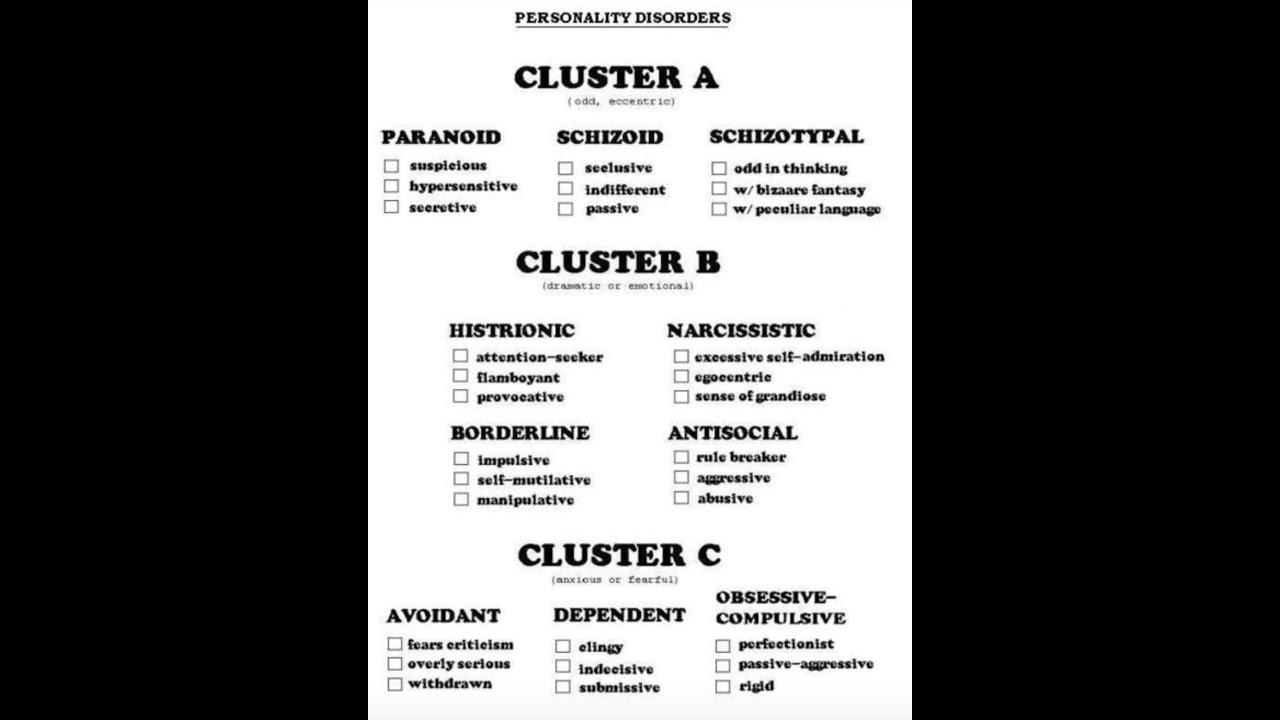
6) Personality Disorders
Not particularly important but good to know, especially borderline personality disorder.
First of all, divide them into three clusters, cluster A, B & C.
7) Psychiatric Emergencies
Neuroleptic Malignant Syndrome, Serotonin Syndrome,
8) Old Age and Organic conditions of psychiatric symptoms
Study about Delirium!
Delirium vs Dementia,
Alzheimer's Disease and its differentials(lewy body dementia, etc)
Other organic causes.
Always rule out other organic/medical/surgical causes
before diagnosing a psychiatric condition!
9) Child and Adolescent
Autism Spectrum Disorders(including asperger's)
ADHD
Conduct Disorder vs Oppositional Defiant Disorder
10) Management of psychiatric conditions
When you present, always start your sentence with: I would like to manage this patient based on the biopsychosocial model....
Bio is basically your pharmacological management.
Combine psycho and social when you present.
Read about psychotherapies which include:
Cognitive Behavioral Therapy(CBT), family therapy, group therapy
Again, read about ECT(indications etc)
Read CPG when you have time!
For me, I depended largely on:
1) https://mzhtb-tor.com/?page_id=373 (download link)
Mastering Psychiatry by Melvyn WB Zhang & Co.(singapore)
2) First Aid for Psychiatry Clerkship
3) Malaysian CPG
Jia you :)
Yours sleepy-ly and hungry-ly,
Kai Bin
No comments:
Post a Comment